A patient presents for planned sterilization via bilateral excisional vasectomy.
What CPT® and ICD-10-CM codes are reported?
A 45-year-old female presents to the ED with chest pain. The provider has an Albumin Cobalt Binding Test to determine if the chest pain is ischemic in nature.
That lab test is reported?
A patient undergoes an MRI of the lumbar spine without and with contrast for left-sided low back pain with sciatica.
What CPT® and ICD-10-CM codes are reported?
A 42-year-old male is diagnosed with a left renal mass. An abdominal incision along with rib resection is made to expose and access the kidney. The left kidney is removed, along with surrounding fat, adrenal gland, lymph nodes in the area, and the incision site is sutured. What CPT ® code is reported for this procedure?
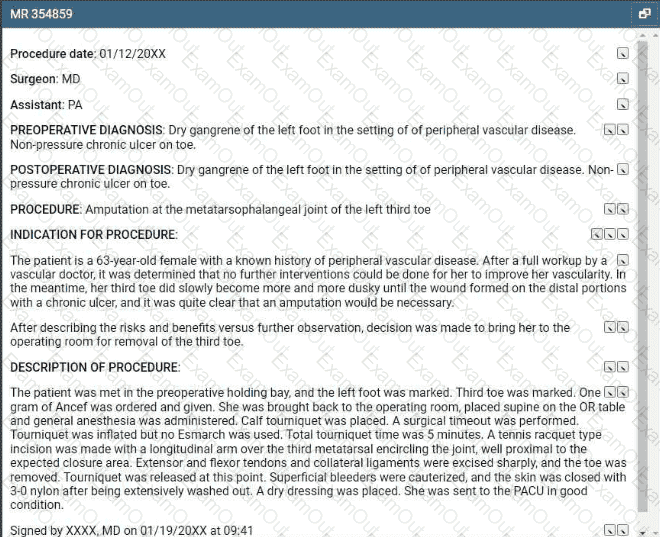
Refer to the supplemental information when answering this question:
View MR 354859
What CPT® and ICD-10-CM coding is reported?
A patient suffers a ruptured infrarenal abdominal aortic aneurysm requiring emergent endovascular repair. An aorto-aortic tube endograft is positioned in the aorta and a balloon dilation is performed at the proximal and distal seal zones of the endograft. The balloon angioplasty is performed for endoleak treatment.
What CPT® code does the vascular surgeon use to report the procedure?
Which is a TRUE statement for Place of Service (POS) codes for professional claims?
Which punctuation is used in the ICD-10-CM Alphabetic Index to identify manifestation codes?
A patient undergoes right thyroid lobectomy for malignancy and removal of a suspicious parathyroid gland.
What CPT® codes are reported?
A patient has five biopsies performed on the duodenum.
What CPT® coding is reported?
