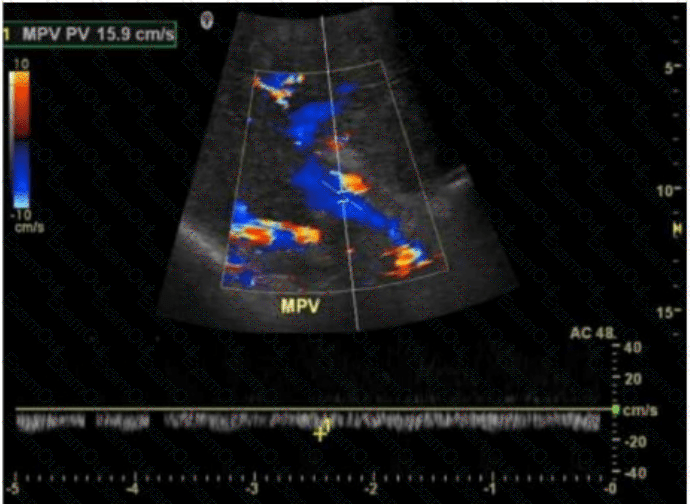
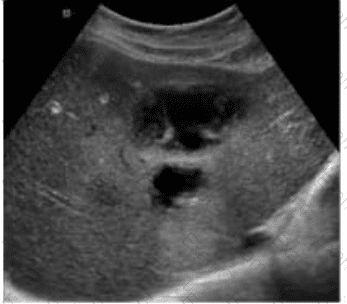
The ultrasound image demonstrates a tubular, anechoic structure coursing anterior to the left portal vein and heading toward the anterior abdominal wall. This is consistent with a recanalized umbilical vein, which is an important collateral pathway that reopens in cases of portal hypertension.
Normally, the umbilical vein becomes obliterated after birth and forms the ligamentum teres. However, in the setting of significant portal hypertension, the umbilical vein may recanalize and serve as a collateral route to decompress the portal system.
Sonographic features of a recanalized umbilical vein:
Anechoic, tubular structure in the ligamentum teres fissure
Seen anterior to the left portal vein
Color Doppler confirms hepatofugal venous flow
Associated with signs of portal hypertension (e.g., splenomegaly, varices)
Differentiation from other options:
A. Budd-Chiari syndrome: Involves hepatic vein outflow obstruction; ultrasound shows absent or narrowed hepatic veins and may have caudate lobe hypertrophy.
B. Splenic artery aneurysm: Typically visualized near the splenic hilum as a pulsatile cystic mass; Doppler shows arterial flow.
D. Median arcuate ligament syndrome: Involves compression of the celiac axis; best assessed with Doppler showing elevated velocities on expiration.
[References:, Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018. Chapter: Portal Hypertension and Collaterals, pp. 101–104., American Institute of Ultrasound in Medicine (AIUM). Practice Parameter for the Performance of a Vascular Ultrasound Examination, 2020., Radiopaedia.org. Recanalized umbilical vein: https://radiopaedia.org/articles/recanalised-umbilical-vein, , ]